Breastmilk production is a simple supply and demand system. Increasing demand will increase milk production. If medical reasons for low or reduced milk production have been ruled out, the combination of the following recommendations are well-known to establish and boost milk production. Yield is dose related *milk removed = milk made*
First Food For Baby is dedicated to providing access to education and lactation care to breastfeeding families. If you are struggling with breastfeeding or have questions, First Food For Baby is here to help.
First Food For Baby Copyright © 2011 – All Rights Reserved / May be used with permission: rene@firstfoodforbaby.com
- Spend as much time as possible skin-to-skin with baby. Wear your baby. Share sleep with baby if you fit the ‘safe sleep 7’ guidelines. Avoid swaddling.
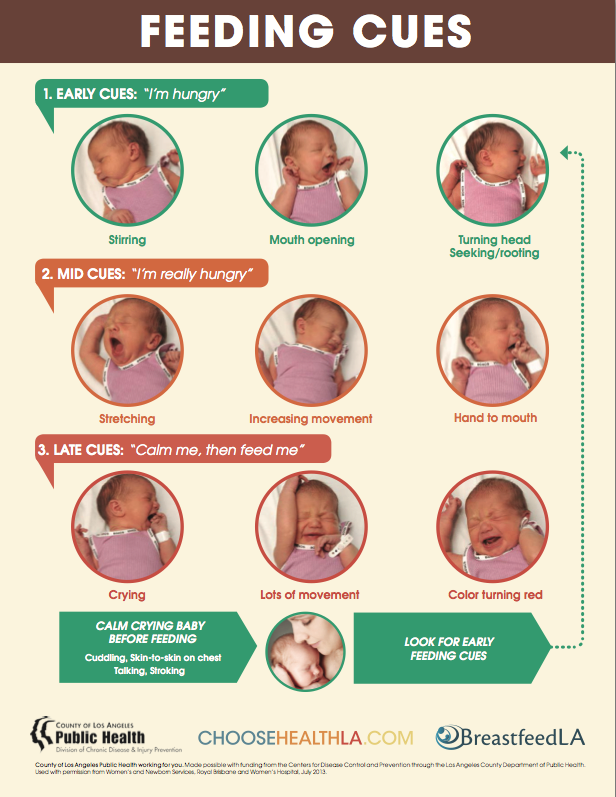
- Feed often observing earliest hunger cues, around the clock. Wake at 3 hours if necessary during the day and at 4-5 hours at night.
- Gently massage breasts right before latching or pumping. Insist on a deep latch and re-latch if necessary. Use breast compressions throughout breast feeds. Use a rental grade pump from the hospital and the correct size breast shield (flange). Consider at-breast supplementation for a few days/weeks (with IBCLC guidance).
- Either pump after a breast feed or pump again within an hour. Empty breasts often, every 45 minutes is not too often at first. You are basically mimicking a growth spurt.
- Repeat. Feed again. Pump again. More skin-to-skin…
- Limit pacifier use or discard if possible
- Try to get 1-2 more feeds in each day especially if weight gain is of concern
- Reduce baby’s crying as much as possible
- If early hunger cues were missed begin the feed alternatively with a small cup, spoon, syringe or bottle to help calm baby
- Follow immediately with a neck snuggle with baby skin to skin up under your chin
- When baby begins rooting latch again
- Include hands on pumping for maximizing milk production
- Using a warm compress will help yield more milk
- Mothers can typically express more milk with hand expression than they can express with insurance provided pumps, especially in the early days
- Boosting milk is hard work but is easier accomplished sooner after birth than later
- Continue to express your milk until your baby becomes proficient at breast
First Food For Baby is dedicated to providing access to education and lactation care to breastfeeding families. If you are struggling with breastfeeding or have questions, First Food For Baby is here to help.
First Food For Baby Copyright © 2011 – All Rights Reserved / May be used with permission: rene@firstfoodforbaby.com
 RSS Feed
RSS Feed

{kind=link}
{kind=link}